2016 Global Digital Health Forum, December 13-14
Session List
| Event | Date(s) | Attendees | Notes |
|---|---|---|---|
| Global Digital Health Forum | Dec 13-14, 2016 | ||
Interactive Session: Data Visualization Tools for CHW Supervision to the Last Mile | Dec. 13, 2016 | Mobile Medic Better World By Design - student run competition for design Toolkit for community health data collection Health facilities, management offices Open source Basic or smart phones, structured SMS or SIM apps Smartphone app - android Data aggregated in web app, then exported to white label tool called Portfolio for data visualization Supports 12,000 frontline health workers → serving 8 million people 55 partners in 23 countries Analytics Percentage goals can be difficult for CHWs to understand Portfolio - white label, buildable widgets, data visualization and performance management tool MedicMobile - non profit, open source Greenmash UK-based Launched in 2011 to address issues in the field Built on mango mobile app platform Operating in Cameroon, DRC, Nigeria, Ghana, Kenya, Tanzania, Somaliland, Madagascar, Uganda and S. Africa Mango: Data capture and workflow/reporting. Also real-time financial transactions. Open API, quick to deploy & share data between Mango & DHIS2 Issues: Speed of data capture & generation of meaningful reports Multiple types of visualization. Graphs, charts. Dashboards, reports Payments Supply chain management - start w/requirements, programs, reporting, users. Commodity tracking - schedules Uganda, DRC Cameroon national malaria control program Quantity tracking, match to disease prevalance JSI Madagascar - linking CHW with resupply points 20 essential meds Send message, let me know what your stock levels are Message/SMS-based. Not necessarily form-based. Flexible? Sloppy? Takeaway: Sounds like it’s trying to be anything for anyone. Look more into partners and implementations. Trying to be ultra-flexible, comes off as disorganized. Asked about supply chain management - response was that facilities/workers can be sent an SMS requesting stock status. Asked for clarification on forms - response was overly-generalized - can create forms, or messages, whatever you want!
| |
The Digital Health Knowledge Base - Content, and Taxonomies, and Platforms, Oh My! | Dec. 13, 2016 | Principles for digital development - if our hypothesis that donor organizations are incorporating these principles into their work, we want to provide resources and documentation Be able to take these 9 high level principles and put them together into a toolkit NetHope, Frog Design Do you need an 80 page PDF? Requirements? Interactive platform? What are the components? Knowledge assets, services, community Helpful for donors/funders to have guidelines - able to share those with recipients in order to guide and direct work streams Apollo Temu - BID Initiative Pilot in Arusha, Tanzania What has been response of people in user groups? Creates ownership/belonging - start in 1 district, move through to others. Discover challenges, bringing people from various discussions. WHO Guidelines for Digital Health 6-8 months, concrete recommendations on what works/doesn’t Implementation toolkit Working with MOHs to design - 13 countries, to prioritize Idea of having a user in mind when building and including Repurposing/reusing - using content that was drafted previously Community of experts, giving credit in application Devising questions based on PICO Have finished questions, have released as a global survey 340 globally have participated 15 questions - 3 that aren’t popular have to do with global $ People want templates, they want something they can use | |
OpenHIE: Global to Local | Dec 13, 2016 | Session presenters and description Session focused on Tanzania’s OpenHIE work. Customizing global solutions to address challenges which have developed organically. Governance will be needed for each registry to maintain on an ongoing basis. Types of registries Immunization registry Client shared registry Facility registry Terminology service (associates/maps codes for vaccines/products) HMIS (DHIS2) Health Worker Registery (not clear if this was there) Data capture
Henry Mwanyika, PATH Tanzania - want to build on the current initiatives, solve duplicate efforts (entry and sources), quick decision making from different levels. What is the future? To have information at our fingertips and integrate existing systems. Ed at INSTEDD will talk about the facility registry Health facility portal (made by a local team). Can download the data (made it public) Hfrportal(facility portal) Planwise (is used for planning supply replenishment)
Carl Leitner, IntraHealth Immunization record, client registry Connectathon with Dlab in country to build capacity of local developers. Sounded like a really good idea for creating buyin and understanding. Derek Ritz
Role playing and acting out a baby's birth.
Rebuilt paper forms so a machine can scan and record transactions (versus typing into a tablet) Scanning saves time and allows for the immunization registry to be used for care management versus recording what happens. Brian, talking about VIMS Transaction traffic is standards based… Interoperability layer (need to check with team on status of VIMS)
Ministry of health of ICT created the health facility registry | |
New Resources from the World Health Organization (WHO)/Johns Hopkins University Global mHealth Initiative (GMI) Partnership | Dec 13, 2016 | Session presenters and description Dykki Settle from PATH elaborated on “A Global Good” — a tool used by numerous countries and funded by numerous donors; easy to implement; adaptable to country-specific needs; well-documented; “packaged for accelerated re-use”; easy to scale; interoperable with other Global Goods. He cited DHIS2 as an exemplary global good. If the tools you are using are not supported, not global goods, then your investment is at risk. Audience examples: OpenMRS, OpenLMIS, master facility lists, the MAPS Toolkit, the OpenHIE blueprint, DHIS2 (especially its ability to scale) Garrett Mehl from WHO unveiled a new resource, the Digital Health Atlas. It is a global atlas of digital health implementations around the globe. For VillageReach and our OpenLMIS work, it offers a way to monitor the trends in different digital tools. In the countries where VillageReach works, it may help us improve coordination and find new partnerships. The Atlas is a new resource that is starting out empty and it is now open and ready for anyone to log in and post the work they are doing. Alain Labrique from Johns Hopkins shared a new joint publication Monitoring and Evaluating Digital Health Interventions. Tigest Tamrat also shared in-progress WHO Guidelines. And Garrett Mehl promoted a taxonomy. | |
Broadband Commission Digital Health Report | See session presenters and description Ann Aerts from the Novartis Foundation shared a preview of the upcoming report:
| ||
Enabling Interoperability | See session presenters and description Katherine (Katie) Healy from Johns Hopkins presented a pilot of mobile health interventions for infant vaccine reminders and scheduling. They also created a digital vaccination register that resembled the previous paper registers and piloted these in Bangladesh. They chose OpenSRP to scale this system to the national level. They also leveraged DHIS2, Tableau, CouchDB, and other tools. They created a standardized “concept dictionary” to store standard terminology and allow data sharing. They created this concept dictionary in OpenMRS. MVP-CIEL is the default dictionary in OpenMRS. It has 60,000 existing concepts and maps to SNOMED, RxNorm and other standards. MVP-CIEL handles concept requests and additions. It allows translations to be gathered.
Alex Little from Digital Campus moderated the questions. Key take-aways:
| ||
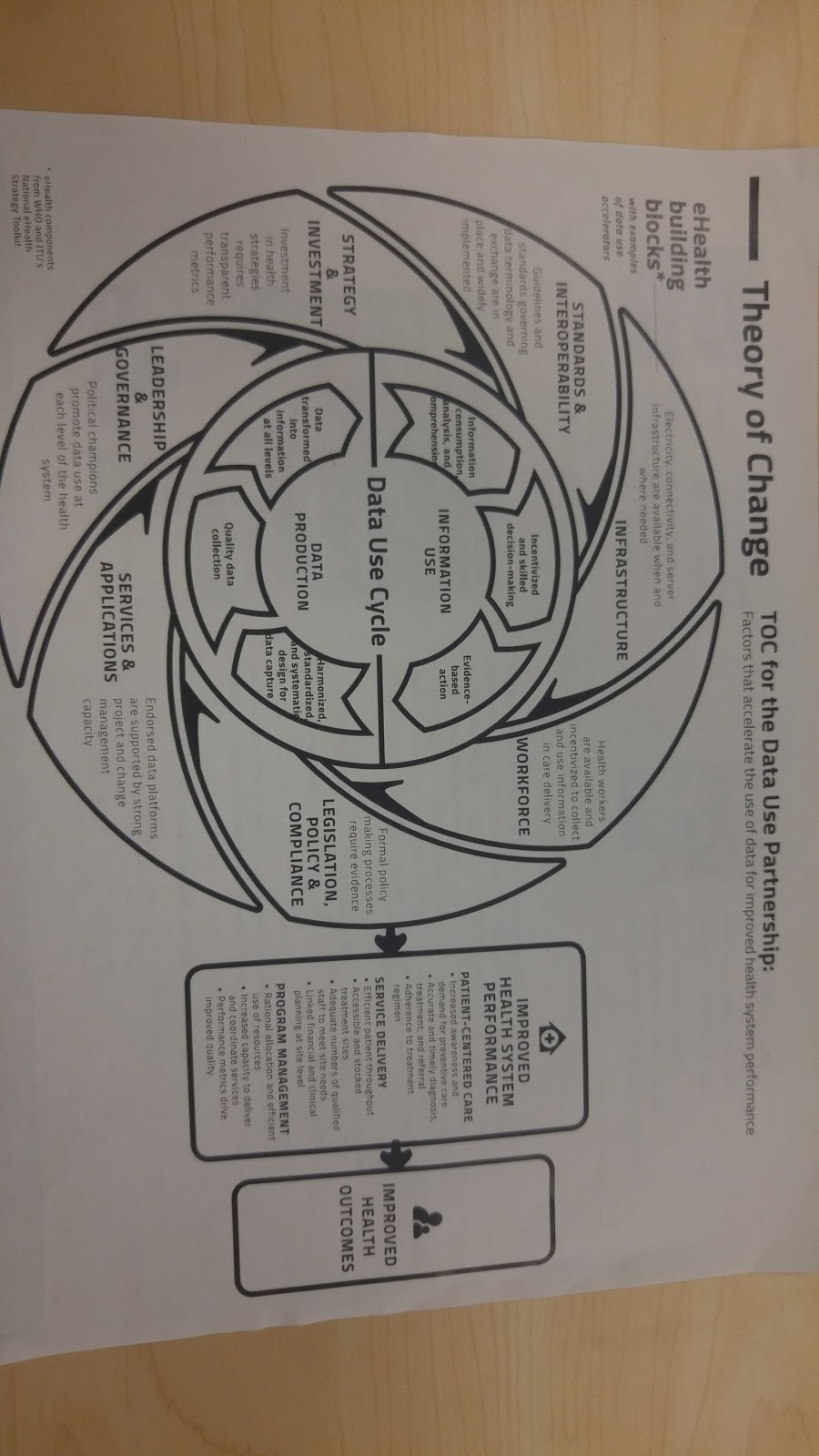
Mapping a Data Use Culture | See presenters and session description I, Mary Jo, arrived late so missed Zambia’s presentation Path’s hand out on Theory of Change and formulating a data culture Malawi & Cooper/Smith The Kuunika project - mapping data use An effort to digitize, currently mostly in paper Kuunika means "to bring light" (ironically used a similar globe for demonstrating "link fragmented systems and expand supply of key health data" 9 goals
Example systems in Malawi (see picture) Baobob health for HER cStock Main issues:
Data use study (see picture)
Framework used (user, element, system to make decisions) Focused on demand of information and what they currently are using Creating a relational database to map the elements to the 9 project goals 5 systems (managing HIV systems) 3,527 elements The right data, in the right format, right person… Optimizing health outcomes within the framework User (incentive alignment, capacity and skills development) System ( infrastructure, system dev, interop/linkage, access tools) Element (better definitions, streamlining, data quality tools Decision (standards, decision support) Systems and sources 185 unique systems Prioritization of decisions for sure! Check this out! This type of effort allows the ministry to focus effort/investment Understanding relationships and data Sankey diagrams (flow diagrams) see website for details on the relationships. Ironically Register and Report are the Source type versus DHIS2 and frequency. Why isn’t DHIS2 being used? Where do we focus? See the 'so what?' section of the website talks about the next steps. Panel from Tanzania, Malawi, Zambia Tanzania
Malawi Woman
Man
Zambia
Marasi asked a question on data quality. Asked the panel to comment on that. Malawi
| ||
OpenLMIS Session | Audience Examples of Customization/Extension Points:
Audience Questions:
| ||
Lessons Learned for Sustainability | Session presenters and description Jeanne Koepsell from Save The Children (and also a conference organizer) introduced the session. Julio Pires from Jhpiego Mozambique and Manuel Macebe from the Mozambique Ministry of Health presented lessons from a Mozambique HRIS implementation. They call their implementation eSIP-Saude. It covers health worker staff records and connects with the payroll system. They had to work across ministries (MoH with civil service and finance ministries). They have a national state employee registry called eCAF. They added health-specific requirements to eCAF. They host the eSIP-Saude in a data center within the country. They showcased dashboards for decision-making and BI. Julio stressed why they pursued collaboration with other ministries rather than doing their own system: they really wanted to leverage existing infrastructure and ensure long-term ownership of the project and the involvement of key players. Collaboration was definitely harder—there were different priorities and different “work rhythms” and methodologies to bridge—but hopefully the long term sustainability makes it worthwhile. He credits their success overcoming this to “win-win approaches”, clear SLAs and NDAs, and alignment with the objectives and interests of all actors. Plus four helpings of patience, according to Julio. He cited the advantages including a faster national roll-out and decreased operational costs. Julio suggests beginning the collaboration at the technical level, but formalizing it at the higher level (inter/ministerial). Erica Layer from D-Tree International presented about the Safer Deliveries program in Zanzibar which works on maternal and child health. Key to program success was closely supporting community health workers and their supervisors.
| ||
Telling Stories with Data Visualizations | Dec. 14, 2016 | see session presenters and description Aly Azhar from VaxTrac shared a Benin case study. VaxTrax is a non-profit with projects in Benin, Nepal and Sierra Leone. Their project, VaxTrac Monitor, created a data dashboard that merges data from clinics up to the district level. Aly showed a Google Map-based dashboard that color-codes each facility to identify which have submitted immunization records recently (green) versus which have not (yellow or red). This map helps MoH staff and supervisors target their follow-up. Aly encourages iterative testing and feedback of dashboards to tune and refine for the needs of users. It was also a challenge to get users to incorporate it into their regular workflow; even though they were initially excited, usage fell off and follow-up was required. Technology-wise, they use an Android app on tablets at health clinics. Data syncs to CommCare. Jeff Bernson from PATH spoke about how visualization of data improves use of data. He works in malaria elimination, and is working in southern Zambia on an initiative called “Visualize No Malaria” with Tableau and the Zambian government. He says “Surveillance is the next malaria vaccine”. Their dashboards help to show what facilities might have missing data. They also created a map visualization to show how community health workers are connected to their community health facilities. Showing this to people on a map helped them see missing data and data errors—it helped all stakeholders realize the importance of engaging district staff to manage their master data. Currently they are experimenting with weather data and maps of where water flows and ponds. By working with MapBox they have started extracting structures from maps and imagery and overlaying all this together. These layers and model help the district staff begin to think about resource allocation. Technology-wise, data is collected on feature phones and flows into DHIS2. They have worked with Tableau to make dashboards and also used Twilio to automate SMS alerts. “Does an SMS count as a data visualization?” For him, it was just as important to get SMS messages out, because the dashboards themselves would not be seen by the specific workers where it mattered. Mandy Dube from PATH also shared stories from the BID initiative about why it is important to make the health worker the hero. | |
Data Moves at the Speed of Trust | Current landscape:
Data lifecycle (see photo)
Risks (see photo) | ||
Understand, Apply, and Expand on DHIS2 | December 14, 2016 | Tenly Snow (Deactivated) | Nicola Hobby - DHIS2 DHIS2 Demo site Shows full range of available DHIS2 offerings Login: admin PW: district Types of data collected: Aggregate data, events, tracking (equipment, drugs → ?) Why is DHIS2 successful?
Data integration driver Can have separate instances of DHIS2 (example DRC MSH, MOH, MSH headquarters), integration driver will pull data from source to destination automatically and in a scheduled fashion. March 23-24, 2017 US-Based, University of Olso-sponsored Bringing together variety of use cases. Used to be NGO-specific, why not open to country use-cases. Interoperability as theme. In DC, FHI360 center. |
CommCare Case Studies | See session presenters and description Lisa Noguchi from Jhpiego showed off a mobile app project to create a tool, powered by CommCare, that helps collect data points to estimate the gestational age in order to better estimate the date of delivery for babies. Sarah Hodsdon from Dimagi showed a project in 5 provinces of Mozambique. Their goal was to identify patients and keep them in monthly treatment for 6 months. Their workflow connects CHWs with case managers at the clinic level. The app is built with CommCare and includes data collection and also the delivery of video content. | ||
Building on Local Capacity and Sustainability | See session description (presenters are wrong there) Presenters: Kathy Gettelfinger, ThoughtWorks; Sean McDonald, FrontlineSMS; Darlene Irby, Palladium; Merrick Schaefer, USAID; Steven Wanyee Macharia, IntelliSOFT; Rebecca Saxton-Fox, USAID. Rebecca Saxton-Fox from USAID announced the creation of WAHIT, the West Africa Health Informatics Team. They are starting a local hiring process now so they can begin to support local HIS tools starting in 2017. → We should explore if we can collaborate with them in an OpenLMIS deployment to get local dev staff. Merrick Schaefer, USAID, described his experience trying to hire local IT/software talent in-country in Africa. He felt it was a “seller’s market”. He also argued that hard skills totally mattered over soft. He also described a large network of Tech Hubs in Zambia, Lagos, and more. Steven Wanyee Macharia, IntelliSOFT, described boot camps and partnerships with universities that are helping to develop more talent. → Connect with Steven by email to get introduced to some of the University of Dar folks, and UW and UCSF folks he is working with. They are implementing Bahmni for EMR needs in Zambia and work in Tanzania and other countries in the region. Sean McDonald, FrontlineSMS, has run a program for 6 years in Nairobi. He argues for a long-term strategy. They offer paid internships and work closely within the community. Successes:
Failures:
Lessons:
| ||
Hindsight is 20/20: Lessons from Mobile Technology for Community Health (MOTECH) program in Ghana | Session presenters and description Anitha Moorthy, Grameen Ghana, described the MOTECH project with its messaging (Mobile Midwife) and data collection components. David Hutchful, Grameen Ghana, described the technology infrastructure. Once a nurse and client meet, data is captured on a feature phone to enroll the client into MOTECH. They may be added to campaigns that provide SMS or Voice messages each week to the client. There are appointment reminders and IVR (interactive voice response). Data feeds into OpenMRS to store all of the actual health and clinical data. Amnesty LeFevre and Larissa Jennings from Johns Hopkins presented about the assessment findings and lessons learned. Tim Wood, now with the Gates Foundation, explained that this project started in 2008 and faced many challenges that are familiar as the global health landscape has evolved: technology, governance, sustainability and more. He specifically noted the lack of early buy-in from Ghana Health Service (the MoH). Issues:
|





OpenLMIS: the global initiative for powerful LMIS software