A page to capture trip notes and photos from the Global Digital Health Forum 2017. December 4-6, 2017, JW Marriot, Washington D.C.
VillageReach attendance:
Conference website:
http://www.globaldigitalhealthforum.org/washington/2017
Conference program: http://exhibitionfloor.himss.org/gdhf17/Public/Sessions.aspx



Day 1: Monday, December 4
An interesting comment by Olasupo Oyedepo, Health Strategy and Delivery Foundation Nigeria
"We need to help the health sector think of tech differently - they should think of it as a tool, the same way a surgeon uses a scalpel. They need to think of tech as a means to achieve health improvements, and we need to help the health sector better communicate their needs to the tech sector."
Alfred, Alpha and the presenters explained the Tanzania current state and future state, including integration between eLMIS and DHIS2 and the LLIN dashboard in DHIS2. They explained the Tanzania OpenHIE framework and work on an eHealth strategy.
Click to expand...
HMIS/LMIS Integration Basics
- Alfred: explains integration DHIS2 and eLMIS; LLIN dashboard in DHIS2
- Alpha: explains TZ OpenHIE framework (with slide diagram); HIM=Health Information Mediator. FUTURE STATE: Interoperability layer routes stock status to DHIS2
- Ssanyu Nyinondi: describes governance and eHealth strategy needed with government
Q&A
- Question: Are private facilities covered?
Answer: yes for DHIS2. But only "ordering facilities" are in eLMIS. Government facilities who get stock from central medical stores.
- Question: What about reporting electronically?
Answer: Of 5000 facilities in eLMIS TZ, roughly 600 report directly.
- Question: Integration uses Batch Files? 1-directional batch updates?
Answer: Monthly batch file from eLMIS is sent to DHIS2 peer-to-peer. But they are now replacing that peer-to-peer with a mediator. The HIM architecture is their future state. For now it uses file with SFTP.
- Question from UNICEF MALAWI : What about when you upgrade the system? Does that break the integration?
Answer: We are working on matching the facilities list and products lists at the Central Medical Stores, which is where the eLMIS workflow ends. We are talking about a new concept: product registry.
- Question: Why not capture the data directly into DHIS2 first, and then push into eLMIS after?
Answer: it is logistics data; DHIS2 is only at the district level. Whereas the logistics data in eLMIS originates at the facility level. The people generating the data are different in both systems. Ssanyu answered: it also involves customizing DHIS2--eLMIS was designed to be implemented at the facility level.
- Question: Is there a national facility registry? National data dictionary?
Answer: HFR is one of the key items. Parts are in operation, other parts on the map are still being rolled out. EPICOR 9 is also in play. eLMIS orders go directly there for fulfillment. In Phase 1 of the OpenHIE integration they are starting with 9 initial systems.
- Question (from Nicola Hobby/BAO): What is the data reconciliation time?
Answer: Some data comes in monthly, but consumption data comes in quarterly. So trying to flatten and reconcile that. Trying to get good reporting rates in both systems so the data will match. So trying to change the frequency of reporting from quarterly to month. That reduces the supply chain cost.
- Question: What about Vaccines?
Answer: VIMS is the 'vaccine module' of OpenLMIS also used in Tanzania and part of the OpenHIE setup.
- Question: Will DHIS2 be able to hold the data from all these different systems?
Answer: For some key use case indicators, we have existing dashboards, so use DHIS2. For now we believe it will be able to support other data.
Quick Overview
Initially they implemented the point to point from HMIS and LMIS
Moving forward they will use the HIE framework. Presented a long-term roadmap
Use case #2a. Interoperability layer will serve as an auditor
Governance with Ssanyu
Needed a body higher up to look at the digital systems holistically.
Governance model to defein
- Policies & Procedures
- HR
- Reporting and Communication (type and frequency)
Financing and long-term maintenance
Ministerial stewardship
Harmonize shared data (facility codes)
Project management office (will review all solutions which come in)
Engagement with ministry is very important for success (at all levels)
Abt associates questions
How did you approach the roll-up?
Answer:
- HMIS roll out first (80-90% coverage by the time eLMIS rolled out) for public and private reporting
- LMIS didn’t include HMIS approach…were only following ordering practices of ordering quarterly. Implementation readiness rather than strategically looking hat harmonizing.
Are there private and public facilities included?
Answers:
- LMIS is the ordering facilities (not private) -> 584 facility level of the total 5,000+ ordering facilities
- HMIS is both
Integration
- Currently, monthly batch file of Point to Point
- Planning to use a FTP
Alfred outlined the key issues
- Facilities sync
- Products sync
- Syncing data
Scott Fitzpatrick question:
- Why push from eLMIS into DHIS 2? Answer: Because Stock data was in eLMIS so that is why it is pushed into DHIS 2
JSI Question: what is the status of shared services of facilities?
- Answer from Alfred: we have the health facility registry
Question on why they decided to eLMIS?
Answer:
- Did a landscape analysis. Looked at Ethiopia but they were switching from that platform.
- Starting 2010 and 11 there was an assessment on readiness. Government drove the decision making and wanted customize it for its own. They enjoyed flexibility with this system. eLMIS can adopt to the shift in processing schedule.
- Also, trying to see how much money facilities can spend on commodities. Are they using all their funds? Tried a peer to peer integration between EPICOR 9 and eLMIS. We want to know the shipment/financial element back into eLMIS.
Question from Nicola on lessons learned.
Answer:
- Data validation and reconciliation process
- Lessons Learned: Cannot reconcile a quarterly consumption to a monthly period.
- Validation that they have high reporting rates (not sure on quality)?
- LMU knows the patterns and consumptions of facilities
- Decide to improve the frequency of reporting
Parambir’s question on transition period or approach to transitioning to the HIE framework.
- Alpha responded (I didn’t hear the response)
Will DHIS 2 absorb all the data and serve as the main data visualization?
Alfred Mchau (Deactivated) it would be great to get the slides uploaded to this page.
by Bayobuya Phulu: MSH/SIAPS (part of the session Digital Technologies Supporting Data for Decision-Making in Africa)
This session showed tools for LMIS, dispensing, and dashboards that were built for SIAPS by MSH – that addresses similar problems to OpenLMIS, OpenSRP, DHIS2, etc.
Click to expand...
Problem:
Pharmacy management tools were largely paper based. Manual aggregation and analysis was a huge challenge with huge turn-around times. This caused poor re-supply decisions; stock-outs of ARVs; hoarding and pilferage.
Solution:
1) Electronic dispensing tool (EDT) and facility electronic stock card (FESC), LMIS reporting & Syspro ERP CSV reports
2) Enhance data transmission - mobile phone network plus USB memory sticks
3) Enhance data processing
Tools and Best Practices:
FESC is web-based (actually he later told me they are re-doing it to be web-based); it has modules for managing stock.
EDT is for patient and stock management at ART sites; it is a Windows application.
–> See both tools here: http://siapsprogram.org/tools-and-guidance/
His slides (slide 9 and 13) show good examples of the (PMIS = Pharmacy MIS). It consolidates data at national, regional and facility levels. They update and use it on a monthly basis! It is comprehensive and timely (much better than paper). Significant features for the ART program as well as for planning (more reliable data for forecasting; facilitates re-distribution and reduces wastage; early warnings for stock-outs and over-stocking).
Slides:
by representatives from JSI, Jhpiego, and Erick Mwale, Save The Children
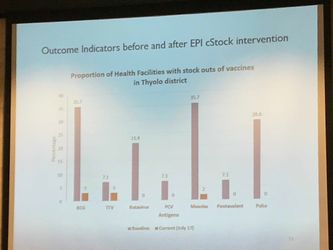
, Save The Children, presented cStock, which used MCSP funding to scale up nationally for EPI in Malawi.
Click to expand...
Problems:
National - lack data; District; Health Facility - stock outs; Community.
Solutions:
cStock transmits logistic information through SMS messages with computer responses for re-supply
- first introduced in 2011 in 6 districts then nationally
- EPI program uses cStock in Malawi with JSI and Save The Children
- using MCSP funding to scale up from the first pilot
- cStock process has a series of meeitngs, orders and responses during the monthly and quarterly cycles
- see also: OpenLMIS notes about cStock opportunities since Dimagi wants to retire cStock: /wiki/spaces/OO/pages/84574228
Results:
improved EPI product availability (reduced stockouts)
Note: Erick Mwale is new at Save The Children. He is based in Blantyre. He was a neighbor of Zachariah Jezman from VillageReach!

Next, Jodi Lis, Jhpiego, presented Digital Learning at MCSP in Ghana
The Hello Nurse app brings game-ified e-learning about Malaria to the last mile in Ghana.
Click to expand...
Jodi explained that they started doing e-learning years ago under MCHIP before MCSP.
- Use Moodle and Moodle Mobile as their open source learning platform.
- they find most people are already familiar with Moodle or have used it before
- it also has an offline mobile mode as well as a Windows client
- midwifery schools are the target users
- work with MOH eLearning Secretariat in Ghana
- trying to get technology into the curriculum in schools
- eLearning content development uses a holistic approach
- with a focus on what the MOH can sustain and keep using later
- Malaria content covers, EG, how to repair a bed net
- Jhpeigo has info on website
- translating content for use in Madagascar next -- lots of work is required in adaption/translation!

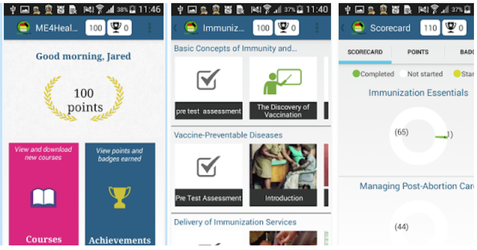
(in Android app store see Hello Nurse and ME4Health)
The website isn't updated with speaker information
- David Nguyen (united solutions)
- Hugh McDonough: Abt Associates
- Maria Vachino: John Hopkins Applied Physics Lab
- Paul Nelson
- Moderator: Kirsta DAI
Click here to expand...
David Nguyen (united solutions) - think about this as a foundation piece of the system. Can reduce the auditing effort/costs. Share data across a complex value chain. Remove the intermediaries.
- I didn’t hear his pitch/speech
Hugh McDonough: Abt Associates
- Exciting to work with something during the hype (retrofit something done into our area)
- Pilot in papua New Guinea, FinTech
- Distributed secure applications were needed (not specifically block-chain)
- Pilot 1: IDBox using fingerprinting to connect people to census services
- Pilot 2: Asset registry app for insurance and loans
- Pilot 3: Vital registries
- Abt is trying to connect the new Tech folks with the field to build their platforms in a way the bottom 2 billion can use their platforms
Maria Vachino: John Hopkins Applied Physics Lab
- Researching block chain for 2 years (capabilities, challenges, etc.)
- Identify management and data privacy for border protection
- Funding research into:
- interoperability
- Distributed key management
- Supply chain management may actually lead to something beneficial because it is permanent and distributed
- Good for supply chain and sensors (IOT sensors)
- Danger around Personal Identifiable Information (anything encrypted will essentially be broken)
- If it needs to be encrypted long-term (quantum computing) - for instance public key encryption will be broken
- Homeland security workshop on benefits and nascent aspects of block chain
- No standard way to read/write to block chain
Paul Nelson
USAID global development lab (focus on finTech)
- I will share more questions I ask start-ups to understand the applicability of this application in USAID
- How does the given distributed ledger “better" than the status quo alternative
- What is the metric is it better by?
- How does it align with the digital development principles?
- How does it account for low resource setting or challenges faced in this sector/field?
Questions
Maria - using block chain for IOT sensors to discover if it has been tampered with
Maersk to IBM (newark to rotterdamn) case studies
Maria - you cannot trust that the ‘right/accurate’ data is first recorded. It only affirms that the data isn’t tampered with after it is written.
Maria - so many of these applications could easily use an encrypted DB on AWS
#you’d be an idiot to put health records on block chain - Maria
What are the characteristics of a problem/challenges where block chain is a good solution?
- Is there a deficit of trust with you are interacting with? Fraud is the biggest reason.
- If you need a legally binding law of transactions.
- If two entities cannot agree on who has legal management over the data.
- Is there a need for the information to be stored in a database?
- More than one person read/writing to the DB
- No viable trusted centralized alternative.
"Testing feasibility and functionality isn’t testing necessity"
Last words
- Hugh: Don’t take block chain in the mind and start thinking what can we do it? Think of a problem and work the possibilities.
- David: Imagine a future where your phone and computer had a distributed ledger. Create a frictionless way for devices to work together. To execute transactions on our behalf. It isn’t block chain alone. The notion of absolute privacy is no such thing. What are willing to give up to derive the benefit.
- Maria: I’d arge that’s an encrypted data store not a ledge. I’d argh not putting sensitive information on distributed ledgers on public encrypted keys. Refugees are more sensitive or vulnerable (which we aren’t aware or are privileged enough to not notice).
- IBM guy: define networks with 3rd parties (not sensitive) and determine what the problems are before saying it has to block chain
- Paul: It is an early stage technology. Unfair to really know clearly where it work and where it doesn’t. Would be valuable if the innovators were being more constructive with implementers.
- Krista from DAI
Open Source: What does it mean, Whom does it serve? A panel to demystify the meaning, use and value of open source software in the digital age.
http://exhibitionfloor.himss.org/gdhf17/Public/SessionDetails.aspx?FromPage=Sessions.aspx&SessionID=2656&SessionDateID=26
- Carolyn Florey DIAL: ICT4D at the Rice Research Institute
- Dykki
- Sharon: Medic Mobile
- Marc: D-Tree
Click here to expand...
Dykki: open source definition on wikipedia. Make it as open and freely available as possible (some rights reserved)
- Free redistribution
- Include source code
- Must allow derivative works
- No discrimination
- Technology neutral
Why is it good for international development? Arguably it is about building capacity and building ownership in country. Adaptable. Not being locked in. Neat alignment between the efforts.
Carolyn: principles came from a series of workshops (open innovation, source, standards, etc.) DIAL started reviewing what has been done.
- Follows the product life-cycle
- Analyze plan
- Design develop
- Deploy
- M&E
- How doe you feel about removing the ‘mandate’ of creating open source? Being more context specific… may not always make sense.
Sharon:
- Just because our code isn’t there doesn’t mean it is accessible
- Open source design methodologies
- Financials are open
Marc: Widely available, cheaper, better?
- Sharon: see it as a way to achieve scale and reach. Lowers barriers to adoption of our toolkit. Hopefully spur innovation. However, doesn’t really materialize without a lot of effort of those who created the original code. We have contributed code back to ODK and ENKATO. End goal is a government to own and manage the tool long-term.
- Dykke: Total Cost of Ownership is not cheaper than commercial counterparts. Money is either going back to license/developers versus into your own country building the capacity of your own team. Community is a ‘wonderful’ by-product.
- Carolyn: the new standards is ‘softer’ on getting government buy-in.
- Dykke: Oracle was an aggressive push to get in the door. No way governments could sustain the on-going support support and customization. PeopleSoft
- Dykke: I came up around redhat, brought them to IntraHealth iRIS. Felt strongly about the uptake of open-source. Previously donors would push stuff and countries would take ‘anything’. Maybe not single software but more modular so you could plug and play with different open source and commercial software.
IntraHealth/Dave Potenziani: usually has dreadful UI, developer has an itch and creates software. Why should our users have a less than delightful experience when they don’t have cash to pay for it.
Anne from Jembi: open standards. How to maintain it? What about a maturity model for open-source?
Scott Fitzpatrick DHIS 2: liability of the core developers? What about usage at your risk? Are d-tree or Oslo protected?
- D-Tree; no liability if taken and deployed without support of Medic Mobile.
- Dykke: reputation of vulnerable software, people will exit. Culpable enforcement depends on jurisdiction and bodies. Trying to address at the policy level.
Transparency is what is important. True costs of implementations. ‘Don’t have the knowledge to get into the details’.
Dykke: as you mature as a business (country) you decide what is ‘my’ core business. Is it IT or outsourcing?
Nils Kaiser (USAID Guinea) : coming up with sustainable solutions can be challenging for ministries when they don’t understand their own capacities. Budgeting is challenging too. Most of our devices are ‘closed’. Telecommunications is another component of ‘closed’. We need budgeting and financing aspects.
Day 2: Tuesday, December 5
Presenters included Amanda BenDor, PATH; Marcos Mzeru, ICT Officer MOHCDGEC, Tanzania, and Mary Rocheleau, Engineering Manager, Vecna Cares Charitable Trust
Click to expand...
Mary Rocheleau, Engineering Manager, Vecna Cares Charitable Trust
- installed 6 hardened servers at clinics throughout a large refugee camp to track patient records
- interoperable EMR: reports for UNHCR and MOH
-- problem: had independent data collection and storage and generating parallel reports to different organizations
-- NOW: collect the same data, use it to create all reports; lower burden to maintain data
- Q&A: patient record merging based on unique identifiers; currently a manual confirmation of possible matches
- why did they build custom hardware? it was hard.
Amanda BenDor, PATH "Sharing Implementation experiences from Senegal" (presenting for Papa Sokhna)
- GHSA - Global Health Security Agenda covers many countries including Senegal, TZ, DRC; collaborates with CDC
- in Senegal, working to improve surveillance
-- digital tools for surveillance: DHIS 2 (first for TB, HIV, Malaria); plus Lab data feeding into DHIS 2
--- two copies: DHIS 2 MOH and DHIS 2 Lab
-- HSISD = Health and Social Information System Division
--- working at Hospitals!
--- training on ICD10
--- harmonizing data collection forms
-- at the Labs, they are doing mapping/landscaping to identify the equipment and workforce at the Labs
Marcos Mzeru, ICT Officer MOHCDGEC, Tanzania mzeru@moh.go.tz
NOT Mr. Hermes Sotter Rulagirwa, Head of ICT, Ministry of Health, Tanzania
- he also had worked for a software provider/vendor there
- TZ has a national health vision
- one-to-one integrations between systems got to be a mess (including VIMS, eLMIS, DHIS2, etc etc)
- Tanzania HIE "to be" model has a Health Information Mediator and Enterprise Service Bus model
-- use case #1: start with client level data exchange for hospitals (4 key indicators)
-- use case #2: sending aggregate data to DHIS2 including from eLMIS, VIMS, E9 (EpiCor 9 at Central Medical Stores) and HRHIS
-- use case #3: health facility registry data extract to post into Interoperability Layer
- HIM Administrator's landing page
-- started with 5 hospitals and eLMIS
- Questions?: Unique IDs, Data Curation
- ALPHA: These systems were not enterprise-ready when they were first built/deployed.



Health Games: Game Based Learning for Health
Sam Schmader, JSI, presented about game-based e-learning for health in Kenya. They have free, web-based health games with modules ranging from Contraception to Lifestyles to Supply Chain. Expand below for free registration info.
Click to expand...
JSI created online game-based e-learning called Health Games. Below are steps on how to register free. The slides below also show the kind of analytics and tracking that their game platform gives.
Go to www.health-games.org
Use Registration Code 4949
Create an Account
This training uses a tool called Yeepa from Germany. I cannot tell if it works well offline, but still a good example of turning learning into a game and tracking learner achievements.

(Brandon shared this with Joseph for SCOR training and Bull City team.)

Open Source
Panel Tuesday at 2:30 including our own Tenly Snow, Carl Leitner (PATH Digital Square), Michael Downey (DIAL) and Dave Potenziani (IntraHealth).
Click to expand...
Introduction:
Michael Downey, Director of Community, Open Source Center, Digital Impact Alliance at United Nations Foundation
- open source is a "hedge" against maintainer burn-out; to survive organizational strategic shifts over time; single points of failure; to catalyze contribution
- http://osc.dial.community/
Carl Leitner on Financing Mechanisms:
- Deputy Director - Global Goods, Digital Square / PATH
- "let a thousand flowers bloom" -> problem for Uganda in 2014 leading to the moratorium
- "software monocultures" is also a problem -- open source tools that are used in many many places at scale
- OpenHIE solves both -- a blueprint for a way of talking and sharing
- Digital Square includes:
-- governance and advocacy
-- aligned funding
-- global good commons? (WHAT IS THAT?)
-- community coordination
-- GGMM = Global Good Maturity Model
-- was developed with input from HDC Health Data Collaborative team
-- 3-axis maturity model
-- example google spreadsheet for self-assessment: http://bit.ly/2AvjV1z (self-assessment in Google sheets)
--> NEXT STEP: we should test and give feedback on their self-assessment tool
-- "Notice B" for 6 awards totaling $600,000 to help global goods proceed along the GGMM "for sustained development"
-- How do we prioritize limited funding? Demographic data (impact/scale); GGMM; Digital Health Atlas; TCO of GGs
Tenly Snow on OpenLMIS:
Tenly Snow (Deactivated) do you want to add your script and slides?
Dave Potenziani about IntraHealth's new iHRIS Foundation
David Potenziani, Senior Informatics Advisor, IntraHealth International
- "we cannot do it alone and we should not try"
- context: global health worker crisis -- shortage of millions of health workers
- "if somebody gives you a kitten, it's great, BUT it is the gift that eats"
Q & A:
- Documentation: Dave/iHRIS: WE want to write the documentation first, then write the code after we have thought through it.
- Balance building new features versus investing in improving/evolving/sustaining existing platforms?
-- Dave: code bounties and projects are often skewed towards the "new and shiny". BUT you have to realize one of the things that requires care and feeding are the people you have already won over. Taking care of those people is not the glamorous, shiny work.
- Language Barriers? How to overcome? Tenly example of holding events in Senegal to bring in perspectives.
- Dreams for the Holidays: more creative ways to do collaborative funding; start to fund innovation even it might fail; more summer of code type programs; want a stronger workforce in countries to manage these tools.

Day 3: Wednesday, December 6
DHIS2 & OpenLMIS & OpenSRP: HMIS/LMIS Integration Demonstration
Lab Session by VillageReach (OpenLMIS), BAO Systems (DHIS2) and Ona (OpenSRP)
Slides: https://docs.google.com/document/d/1bNoV6T1RZkI8Kkhot6aY4XqKINMedbcvYfT0w9nM3O4/edit?usp=sharing